Ectopic pregnancy is the implantation of an embryo in a position outside the endometrium (usually in the oviducts). It can occur after natural conception at a rate of 1-1.5% (Lensy et al 1999). In IVF programs the incidence is slightly higher.
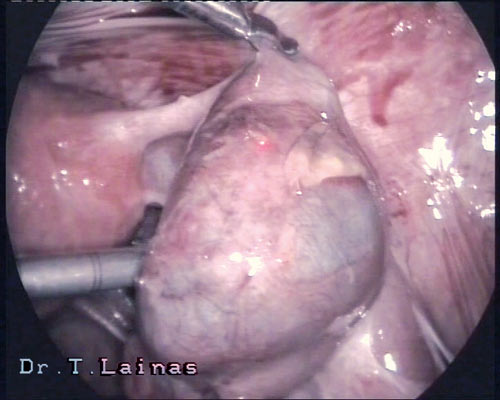
Ectopic pregnancy on right fallopian tube (laparoscopic image).
Depending on the site of implantation, we can distinguish the following types of ectopic pregnancy:
- Tubal pregnancy (approximately 99% of ectopic pregnancies). The zygote may implant in either of the four segments of the fallopian tube (oviduct): interstitial (3%), isthmic (25%), ampullary (55%) and infundibular (17%). The causes may be, mechanical, functional etc.
- Ovarian pregnancy: Implantation happens on the ovary and occurs at a frequency 1:7000.
- Peritoneal pregnancy: Implantation happens in the peritoneum or the intestine either from the beginning or after expulsion of the embryo from the ampulla of the oviduct. It occurs at a frequency 1:8000.
- Cervical pregnancy: Implantation happens in the inner cervix and occurs at a frequency 1:8000.
- Simultaneous uterine and ectopic (usually tubal) pregnancy. This the onset of a rare type of multiple pregnancy (1:10000) and occurs more frequently in IVF programs compared to natural conception.
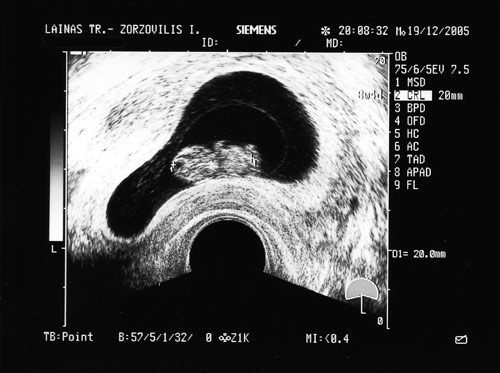
Diagnosis is performed timely and at an early stage (6th week of gestation), as at the first ultrasound examination, that is performed 14 days after a positive hCG test, the exact site of the embryo can be identified.In the past, the diagnosis of ectopic pregnancy was based on symptoms prior to the rpture of the oviduct, and included delay of menstruation, pelvic pain and vaginal bleeding, as well as symptoms after the rupture of the oviduct, which included acute pain and sites of internal bleeding. Nowadays, diagnosis is easy using the levels of beta hCG combined with a vaginal ultrasound.Ectopic tubal pregnancy is treated with laparoscopic surgery, which is now considered the treatment of choice. The traditional laparotomy with removal of the oviduct is a thing of the past, with very few and contradicting indications. Surgical treatment of ectopic tubal pregnancy can be performed by:
- Retaining of the oviduct (salpingostomy). In this case a longitudinal section of the oviduct is performed using laser CO2, followed by aspiration of the fetus. The oviduct is checked for bleeding, and the wall usually seal by themselves without suturing. It is necessary to measure hCG after a week.
- Removal of the oviduct (salpingectomy) is performed when there are indications like rupture of large distension of the oviduct wall.
It is also proposed that the treatment of an ectopic pregnancy can include drug administration, like methotrexate, either intramuscularly or with injection in the embryonic sac under ultrasound or laparoscopic guidance. It is recommended more for cases of interstitial, cervical and peritoneal pregnancy (to induce earlier regression of the placenta, which in these cases is not removed because of the high risk of bleeding).
Management of ectopic pregnancy
Management of ectopic pregnancy using laparoscopic surgery is nowadays the method of choice. Until the 1970s, laparotomy was used due to the inability of early diagnosis, resulting in the rupture of the ectopic pregnancy.
VIDEO: Ectopic pregnancy on right oviduct. Salpingοtomy, fetal removal and retaining of the oviduct.
Early diagnosis is now performed prior to rupture, using beta hCG levels combined with ultrasound examination. Laparoscopic verification is rarely needed. Early diagnosis and laparoscopic surgery have nearly eliminated the disease and mortality due to ectopic pregnancy, and have improved significantly the rate of post-operating infertility.Contraindications for laparoscopic surgery, as reported 20 years ago (Mage G., Canis M., Bruhat M.A) include:
- Absolute contraindications: interstitial pregnancy, shock, opisthoperitoneal hematocele, and contraindication of general anesthesia.
- Relative contraindications: hemoperitoneum >15000 ml, obesity, extensive adhesions.
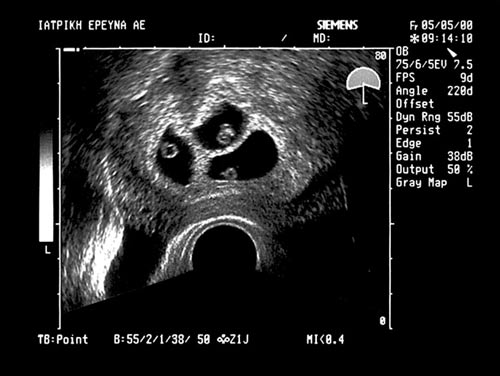
VIDEO: Ectopic pregnancy on both oviducts. Salpingotomy, removal of fetus and retaining of the oviducts.
Laparoscopic surgical treatment of ectopic tubal pregnancy can be either conservative, with longitudinal salpingotomy, aspiration of the fetus and retaining of the oviduct, or radical, with excision of the oviduct.The choice of laparoscopic treatment in based on criteria, but also on the experience and training of the surgical team. The criteria include history of infertility, prior or repeated ectopic pregnancy, salpingoplasty, site of implantation (isthmus, ampulla, infundibulum), bilateral ectopic tubal pregnancy, and risk of oviduct rupture. Based on the score that results from these criteria it is decided whether to retain or remove the oviduct.a) ) In the case of oviduct rupture, laparoscopic surgery involves a longitudinal section 10-15 mm is above the fetus, removal of the fetus using flushing with saline, aspiration of the fetus away from the wall of the oviduct. The oviduct is examined for bleeding and the wall remains open. Rarely are sutures needed. At the end of the operation the pelvis is flushed with saline, all fetal elements are removed from the pelvis and the other oviduct is examined.Post-operating monitoring includes measurement of hCG levels 2 days after the operation, and then every 2 weeks until hCG is no longer detectable.b) In the case of oviduct removal, the operation is performed using bipolar diathermy for hemostasis, and the excision of the oviduct is done using laser CO2 or scissors. The section is performed very near the oviduct taking care not to damage the blood supply of the ovary.See more: Management of ectopic pregnancy