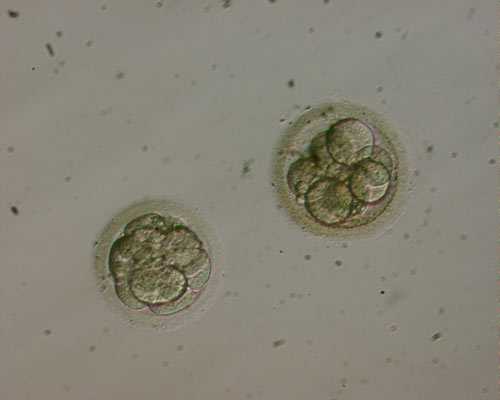
Cryopreservation is the preservation of cells, tissues or even organs at very low temperatures, with the intention of future use. At the temperature of -196oC, metabolism stops and the cells enter a state of suspended animation making it possible to store them for a long time. To achieve such a low temperature we use liquid nitrogen. The first successful cryopreservation was performed in frogs in 1945. The first animal sperm banks operated in 1949. The first successful inseminations I the human were reported in 1953 (preservation in dry ice, -70oC) and in 1964 in liquid nitrogen. Embryo cryopreservation was first performed in laboratory animals in 1972 and in human in 1984.
Today, cryopreservation is a routine method, allowing the storage of gametes and embryos for an extended period.