After the retrieving the sperm sample from the male partner, the sample is prepared to isolate the normal motile spermatozoa. Even a few thousand spermatozoa are enough for ICSI to be performed. Hoverer, in cases with immotile sperm of obstructive azoospermia, the sperm must be retrieved using surgical methods from the epididymis or the testis.
ICSI is performed in two steps. First, the oocytes are stripped from surrounding cumulus cells using a combination of enzymatic (hyaluronidase) and mechanical methods. This step is important for the identification of mature oocytes and for the esae of micromanipulations. Maturity is determined by the presence of the first polar body. Only mature oocytes can be used for ICSI. Immature ones cannot be used.

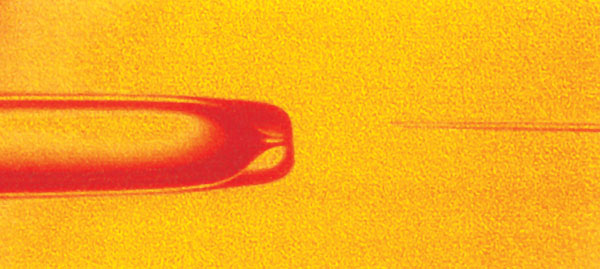
A. Mature oocyte with extruded first polar body (at 6 o'clock). The injection pipette that contains the spermatozoon approaches the oocyte. (Eugonia archive)
B. The injection pipette has penetrated the zona pelucida and the oocyte membrane. The spermatozoon will be deposited inside the oocyte cytoplasm. (Eugonia archive)
The second step is the actual performance of ICSI. The naked oocytes are placed in drops of culture medium in a petri dish and is help in place by the holding pippete. In a different drop, sperm are deposited, and each spermatozoon is immobilized and aspirated in to the special injection pipette. The spermatozoon is then injected inside the oocyte (one spermatozzon per oocyte). Each injection usually lasts for a few seconds, but the entire procedure may take several hours to complete in cases of high oocyte numbers or extremely low sperm numbers.
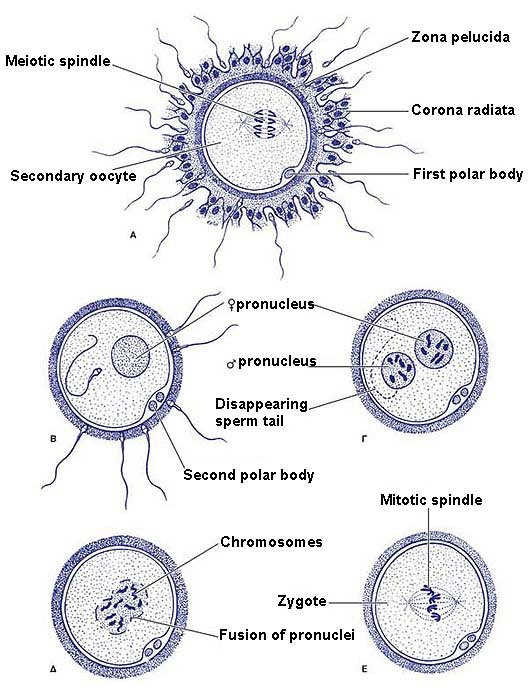
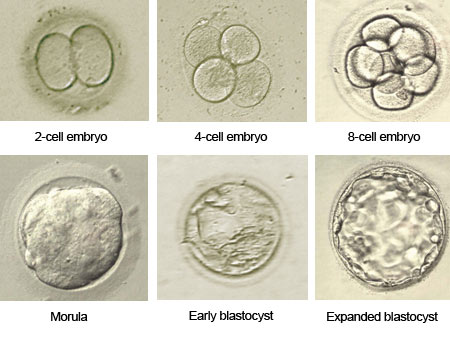
After the injection, the oocytes are placed back in the incubator. Polyspermy is avoided using this method. Fertilization rates are usually high after ICSI (higher than 60%). Fertilization failure after ICSI is usually related to inability of the sperm chromatin to decondense, or abnormal oocyte activation. Damage rates are usually low (2-3% in experienced hands). From that point on, the procedure is the common irrespective of the fertilization method (i.e. formation of pronuclei, cleavage into 2,4,8, etc blastomeres, and embryo transfer).

 Surrogacy applies to couples with normal eggs and sperm but the woman has a non functional uterus or is unfit to gestate for medical reasons.
Surrogacy applies to couples with normal eggs and sperm but the woman has a non functional uterus or is unfit to gestate for medical reasons.