The egg collection is the recovery of eggs from the ovaries. It is performed in a special room in our Unit, under sterile conditions, at a specific time, usually 35-36 hours after the last injection (Pregnyl, Profasi, Ovitrelle).
|
|
|
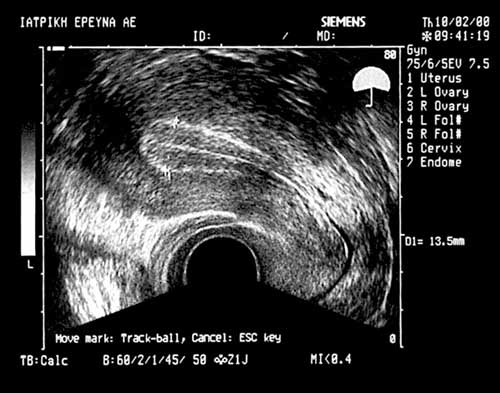
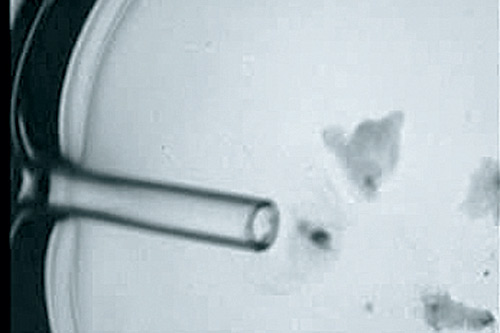
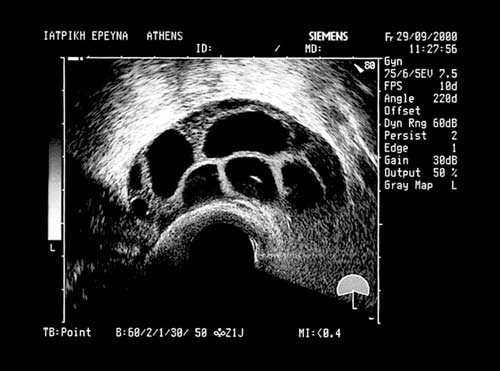
Ultrasound guided transvaginal egg collection. In the picture we can see the tip of the aspiration needle inside the follicle (EUGONIA archive).
|
VIDEO: Egg collection
|
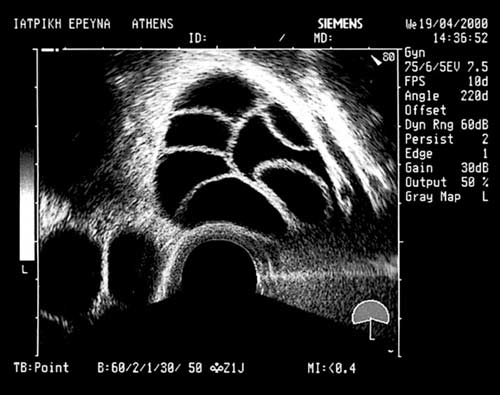
The egg collection is performed by the doctor transvaginally, under constant ultrasound guidance, which facilitates the doctor's precise manoeuvres. The follicles are punctured one after another using a special needle that traverses the vaginal wall.
The contents of each follicle are aspirated into special tubes and are passed on to the embryology laboratory. The embryologist locates the eggs and places them in dishes containing culture medium.
All the equipment and consumables used fulfill special requirements, ensuring that they are not potentially toxic to the gametes and the embryos.
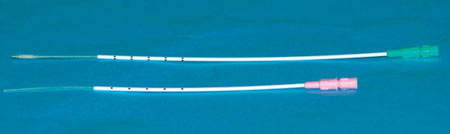
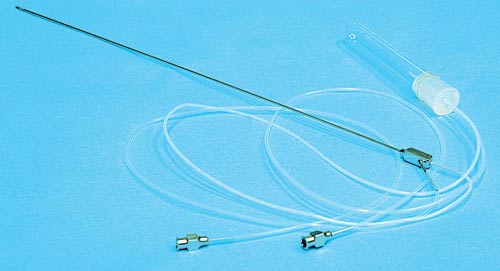
If the egg has not be collected, the doctor flushes the follicle with an isotonic solution (one to three times, until the egg becomes unattached). For this reason, at Eugonia we now only use a double lumen needle with a special inter-lumen connection system that allows the flushing medium to enter the follicle.
VIDEO: Location and collection of an oocyte during egg collection.
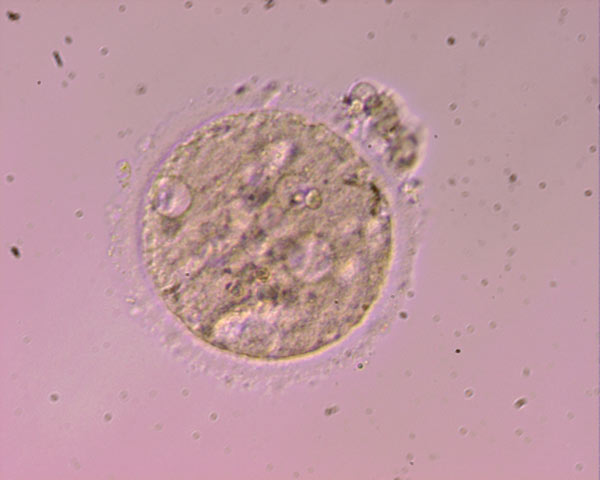
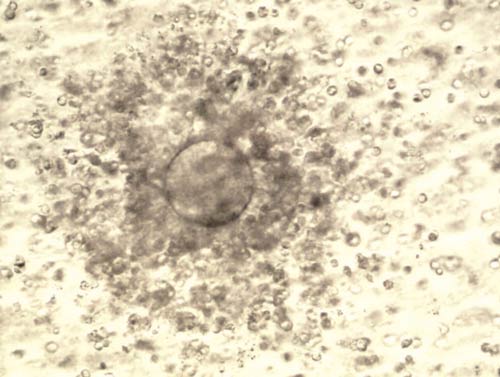
Oocyte surrounded my cumulus cells (EUGONIA archive).
For the follicular fluid aspiration, the needle-lumen system is attached to an electronic aspiration pump with a digital display of the sub-pressure selected. Please note that the eggs are sensitive to the sub-pressure and the adjustment of the pump within certain accepted limits is important.
As we have mentioned before, the contents of each follicle (follicular fluid) along with the oocyte and its cumulus cells are aspirated in special tubes and are passed to the embryology laboratory.
The embryologist locates the oocytes and isolates them in special little vessels called culture dishes, which contain special culture media. All the equipment and consumables used fulfill special requirements, ensuring that they are not potentially toxic to the gametes and the embryos.
The culture dishes are then placed in an incubator under specific culture conditions (darkness, temperature of 37ºC, 5% CO2 atmospheric pressure, 100% humidity). Generally, in every culture dish 1-4 eggs are placed, according to the IVF technique to be used for fertilization (there are certain laboratory variations of this technique that do not affect the events to follow and that is why they are not explained in detail).
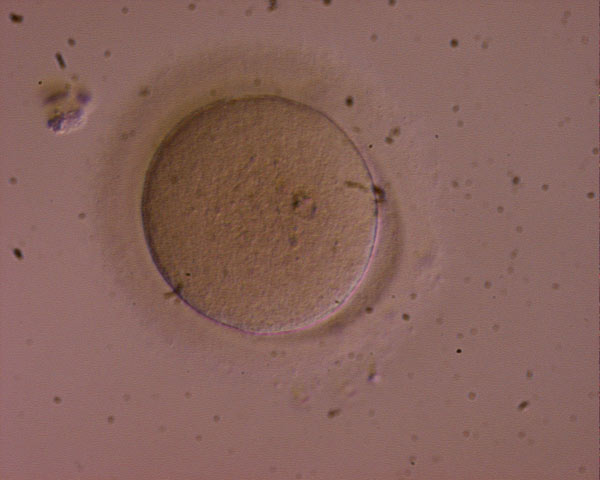
According to the thickness, the size and the density of the cumulus cells, the embryologist can estimate the maturity of the eggs collected.
Except for the maturity of its cumulus cells, the oocyte also needs to be mature with regards to its cytoplasmic and nuclear contents. Despite other cells in the human body, oocytes and spermatozoa contain half the chromosomes (i.e. only one copy of each chromosome in their nucleus). A mature oocyte therefore contains 22+X chromosomes and a spermatozoon contains either 22+X, or 22+Y. When the oocyte and the spermatozoon are combined with fertilization, a cell with a normal nuclear constitution is then created (i.e. a cell that has two copies of each chromosome). A mature oocyte has completed nuclear changes that enable normal fertilization meaning that it has extruded one set of its 23 chromosomes in a small structure called the first polar body which is situated just under the zona pellucida. The presence of the first polar body means that the oocyte is truly mature.
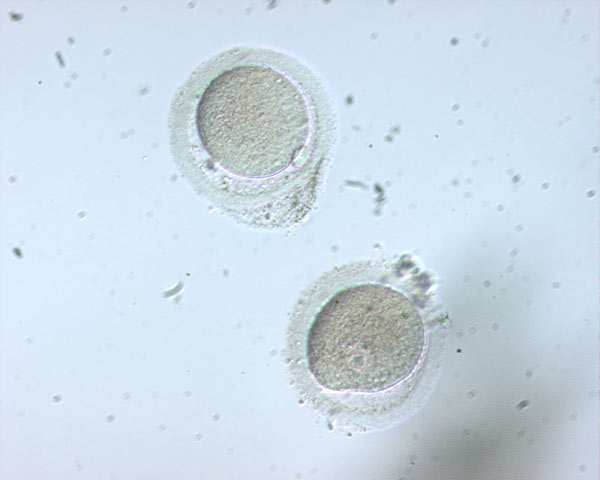
During the use of classic in-vitro fertilization (IVF), the presence of cumulus cells around the zona pellucida is necessary and we cannot check for the presence of the first polar body. In this case, we rely mainly on the morphological observation of the cumulus cells after the egg collection. On the contrary, during the use of intra-cytoplasmic sperm injection (ICSI) the removal of the cumulus cells is necessary in order to check for the presence of the first polar body and the identification of the mature eggs that can be fertilised and also for the ease of the oocyte maneuvering during the ICSI process.
Double lumen oocyte collection, Casmed type (EUGONIA archive) .
Electronic aspiration pump (Labotect type) used for egg collection. The sub-pressure level is selected and adjusted automatically in order to protect the oocytes (EUGONIA archive).