Our pregnancy rates
See more: Pregnancy rates at Eugonia
How pregnancy rates are presented
See more: How pregnancy rates are presented
Pregnancy rates in Europe
See more: European pregnancy rates
Our pregnancy rates
See more: Pregnancy rates at Eugonia
How pregnancy rates are presented
See more: How pregnancy rates are presented
Pregnancy rates in Europe
See more: European pregnancy rates
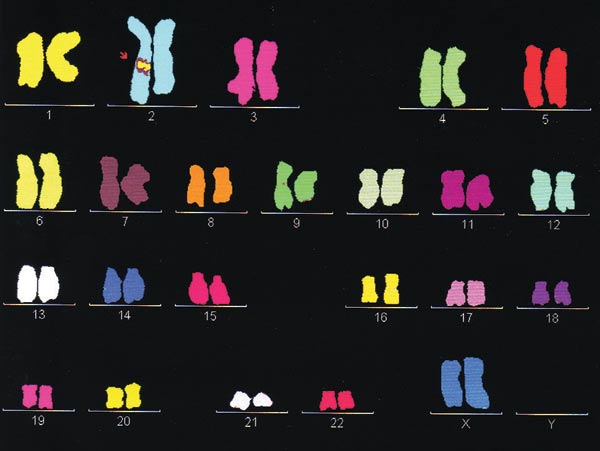
In cases of repeated failed IVF attempts, especially for women of advanced age, in couples with normal karyotype and severe male infertility, or in cases of repeated early pregnancy loss, the embryos may undergo preimplantation genetic screening (PGS). Using special cytogenetic methods (FISH or array-CGH) it is possible to screen some or all the chromosome of each embryo.
Screening one or even two cells of an embryo may not always be accurate, and may be misleading in cases of embryo mosaicism. Mosaicism is a condition in which an embryo may contain both euploid and aneuploid cells.It has been reported in the literature that the application of PGS in women over the age of 35 does not lead to increased birth rates. Despite the skepticism that was associated with these studies, since then the method is less frequently used, and some official bodies like the British Fertility Society have advised against the use of PGS with FISH.A more accurate diagnosis of an embryos chromosome status can be obtained by studying all the chromosomes. Comparative genomic hybridization (CGH) is a recently developed genetic method that studies the entire genome, with very promising results.
It is necessary that all couples who are candidates for PGS seek genetic consultation by a geneticist.
The scientific team at Eugonia has the required training and expertise to offer PGS.
PGD allows the identifications of genetic abnormalities of the embryo while it develops in culture. The method detects certain genetic abnormalities in the embryo, which are responsible for known congenital or hereditary diseases.
Embryos that undergo PGD are biopsied on Day 3 after oocyte retrieval. The embryos are first placed in a special solution to loosen the intercellular bonds. Then a small opening is created on the zona pelucida using laser, and using a special micropipette one cell (blastomere) is removed from each embryo. The biopsied cell will undergo genetic analysis, while the remaining embryo will continue to develop in culture. It has been observed that the removal of a single blastomere at this stage of embryonic development does not adversely affect embryo viability.
With PGD, we identify specific gene mutations (using polymerase chain reaction, PCR), and structural or numerical chromosome abnormalities (using FISH, fluorescent in situ hybridization). The abnormal embryos are therefore identified and excluded from the embryo transfer. Only healthy embryos are selected for transfer in the uterus, at the blastocyst stage on day 5 or 6. If the gene causing a genetic disease is located on a sex chromosome, then sex selection is required to avoid development of the disease in the embryo. This is the only case when sex selection is performed.
Cases that require PGD include -thalassaemia, cystic fibrosis, Down syndrome, etc.Thanks to the continuous evolution of genetic analysis technology, an increasing number of genes responsible for hereditary diseases can be identified, helping us to avoid even more genetic diseases, even some forms of cancer.
PGD has an advantage over conventional prenatal diagnosis methods, ie amnioparacentisis and trophoblast biopsy, as it can avoid potential abortion if the diagnosis is positive for a certain abnormality.

It must be clear that PGD searches for specific abnormalities and does not preclude the birth of a child with a different genetic disease. It is necessary that all couples who are candidates for PGD seek genetic consultation by a geneticist. The scientific team at Eugonia has the required training and expertise to offer PGD for the prevention of genetic diseases.
Before your embryo transfer, the only kind of preparation required is to drink 4 glasses of water without urinating before arriving at the Unit.
You should refrain from using perfume as it may be toxic to the embryos. Remember to bring your Utrogestan pills with you. You can eat normally.
After embryo transfer you must rest in your room for about an hour.
Along with your instructions for medication (usually pills or progesterone cream), you will also be given a picture of the embryos transferred to your uterus. Usually the first pregnancy test is 13 days later (blood sampling for determination of β-chorionic gonadotropin levels).
Implantation of the embryos into the endometrium occurs 4-5 days after day 2-3 embryo transfers and 1-2 days after blastocyst (day 5-6) embryo transfers. Therefore, during these first days after embryo transfer, it is good to avoid physical fatigue, mental tension and sexual intercourse. Missing work is not necessary, provided it is not too tiring. Your eating habits can remain the same.
The reason why more than one embryos are transferred is certainly not the achievement of a multiple pregnancy. Our aim is a single pregnancy by transferring one high quality, chromosomally normal embryo.
However, based on the morphological criteria used to date, it is not possible to always make direct conclusions about an embryo's true quality and developmental competence, nor about its chromosome constitution. It has been suggested that the human is a subfertile species, with 20% monthly fertility rate, compared to primates (80%) or rabbits (90%). It has been shown that 50% of preimplantation embryos have chromosomal abnormalities, and either do not implant at all, or result in early pregnancy loss a few days after implantation.
Chromosomal abnormalities increase with advanced age. For example, a 35 year old woman has a 1/280 chance to have a baby with Down syndrome, while for a 45year old woman the chance is 1/30. Recent studies showed that for women older than 40 years, the possibility of aneuploid oocytes ranges from 60% - 90%, and therefore is the main reason why older women have a lower pregnancy rate. The other reason is that they have a reduced ovarian reserve.
Based on the above, it is clear why we transfer more than one embryos. Our aim is one healthy baby for each couple having IVF treatment. Multiple pregnancies are now considered a side effect, and there is an international tendency to reduce the number of transferred embryos.
An important decision that must be taken after discussion with the couple involves the number of embryos transferred to the uterus. We will inform you about the quality of your embryos before the embryo transfer.

According to national legislation the number of embryos transferred must not exceed three for women below the age of 40, and four for women over 40 years of age. However, this number can be further reduced in special cases (e.g. young woman with good quality embryos) without impairing the outcome. The factors that must be taken in consideration include embryo quality, age of the woman and medical history.
The choice of number of embryos transferred must meet a fine balance between the increasing pregnancy chances, which are usually enhanced by increasing the number of embryos, and at the same time reducing the chances of a multiple pregnancy, which is achieved by reducing the number of embryos.
Internationally, there is a tendency to reduce the number of embryos for transfer to one, as multiple pregnancy is not regarded as a successful achievement any more, but an undesirable side effect of IVF.

The procedure of the embryo transfer is of vital importance for a successful outcome after IVF treatment. Therefore, a careful and atraumatic embryo transfer in skilled and experienced hands can maximize the chances of pregnancy.
The advantages of ultrasound guidance during embryo transfer include:
Future studies and improved methods of guidance (3D and 4D ultrasound), as well as more research on the optimal location inside the uterine cavity to deposit the embryos may increase IVF success rates.
This is the procedure of transferring the embryos back in the woman’s uterus. It is a painless procedure that last for about 10 minutes. It can be performed 2 to 6 days after oocyte retrieval. The embryologist selects the decided number of best quality embryos for transfer, based on certain morphological characteristics (number of cells, size and shape, fragmentation).

The procedure is performed using a special flexible thin catheter, in which the embryos are loaded. After the cervix has been exposed and the vagina carefully washed, the mucus is aspirated. The embryologist aspirates the selected embryos inside the catheter along with minimal volume of culture medium. The gynecologist inserts the catheter through the cervix into the cavity of the uterus under ultrasound guidance. The embryos are then carefully expelled in the uterine cavity. The catheter is then redrawn and checked by the embryologists under the microscope to verify that all embryos have successfully expelled.
This is one of the most important moments of an IVF cycle that is why it is important that the woman is completely calm. The clinical team must be experienced, precise and rapid in order to minimize exposure of the embryos. The correct performance of the embryo transfer is necessary for a successful IVF outcome. After the embryo transfer, the woman must remain in bed for one hour, although this practice is doubted by some studies.
Until recently, oocyte cryopreservation remained a challenge in human IVF, because the low survival rates of oocytes lead to low pregnancy rates. Recently however, the method of vitrification has revolutionized oocyte freezing and it is associated with high rates of oocyte survival, fertilization, embryo quality and pregnancy rates. The method can be also applied on cleavage stage embryos and blastocysts.
Vitrification is a method of ultra-rapid freezing. The oocytes or embryos are placed in special cryoprotectant solutions and then are plunger directly in liquid nitrogen, where they will be stored until later use. In this way, the interior of the oocytes reverts to a form of glass, avoiding the formation of ice crystals that are detrimental to oocyte viability.
Oocyte cryopreservation is performed during an IVF cycle following ovarian stimulation. It is a method of storage of genetic material for women who wish to postpone having a child until later in life, as well as in cases of premature ovarian failure or azoospermia.
According to the Greek law, oocytes can be cryopreserved for up to 5 years.
At Eugonia, we use vitrification for oocyte cryopreservation, following the international scientific developments, informing the patients about the method's advantages and disadvantages.
In Eugonia we have several successful pregnancies following oocyte vitrification.
Theoretically, sperm can stay frozen indefinitely. A pregnancy has been reported in the literature using sperm which had been frozen for 20 years.
Sperm should be cryopreserved:
![]()
Eugonia - Assisted Reproduction Unit
Konstantinou Ventiri 7(HILTON), 11528 Athens
Member of:![]()
![]()
![]()